Intrauterine insemination (IUI) and in vitro fertilization (IVF) are two common assisted reproductive technology procedures (i.e., fertility treatments) that may be offered to couples who are diagnosed with infertility or are having trouble trying to conceive.
Your fertility doctor will take an initial history and obtain a basic evaluation to help determine which fertility treatment may be an option for you and your partner and which one may be best in your unique circumstance.
But what if both IUI and IVF are options?
What’s the difference between them…
And which one is right for you?
Here’s a quick overview of what you’ll discover:
Important Differences Between Intrauterine Insemination and In Vitro Fertilization
One of the biggest differences between IUI and IVF is where fertilization actually occurs…
With IUI, fertilization (insemination of an egg with a sperm) is occurring inside a woman’s body.
With IVF, fertilization is occurring outside the body, in vitro (in a dish), hence the name.
There’s a bit of alphabet soup when it comes to fertility treatments with lots of different acronyms depending on what source you read, so it’s easy to get different infertility treatments confused.
Let’s break each one down in a bit more detail to help clarify!
What is intrauterine insemination (IUI)?
Intrauterine insemination is a process wherein the sperm sample is prepared and washed to get the highest concentration of the most motile sperm into a small volume (usually ~0.5mL) and is then placed directly into the uterine cavity around the time of ovulation.
Around the time of ovulation, the fallopian tube will pick up the egg where it then travels towards the uterine cavity. The sperm meets the egg in the fallopian tube, where fertilization occurs, and the embryo then travels the rest of the way to implant in a woman’s uterus.
Thus, intrauterine insemination is essentially getting a MUCH higher concentration of the sperm closer to the egg by bypassing the cervix completely so it doesn’t have to swim so far! This can be super helpful if your male partner has low sperm count or poor sperm motility.
In fact, of the millions of sperm that are ejaculated during intercourse, only about 200 of the them actually ever make it to the fallopian tube. With IUI, ideally, you have > 10 million motile sperm deposited directly into the uterine cavity thus increasing the chances of getting pregnant.
Women will often take oral ovulation induction medication for 5 days early in the menstrual cycle to boost ovulation along with intrauterine insemination. The most common oral fertility medications used are Femara (i.e., letrozole) and Clomid (i.e., clomiphene citrate).
You can detect ovulation to time intrauterine insemination with ovulation predictor kits (LH kits) or mid-cycle ultrasound monitoring. Your reproductive medicine physician will let you know which option might be best for you (this is also dependent on the clinic’s protocols).
The actual IUI typically takes about 5 minutes. The woman has a speculum placed (just like you’re getting a pap smear) and a small catheter is inserted through the cervix and into the uterus where the IUI sample is then deposited directly. Some women may experience a mild cramp, but in general, IUI is very well tolerated.
What is in-vitro fertilization (IVF)?
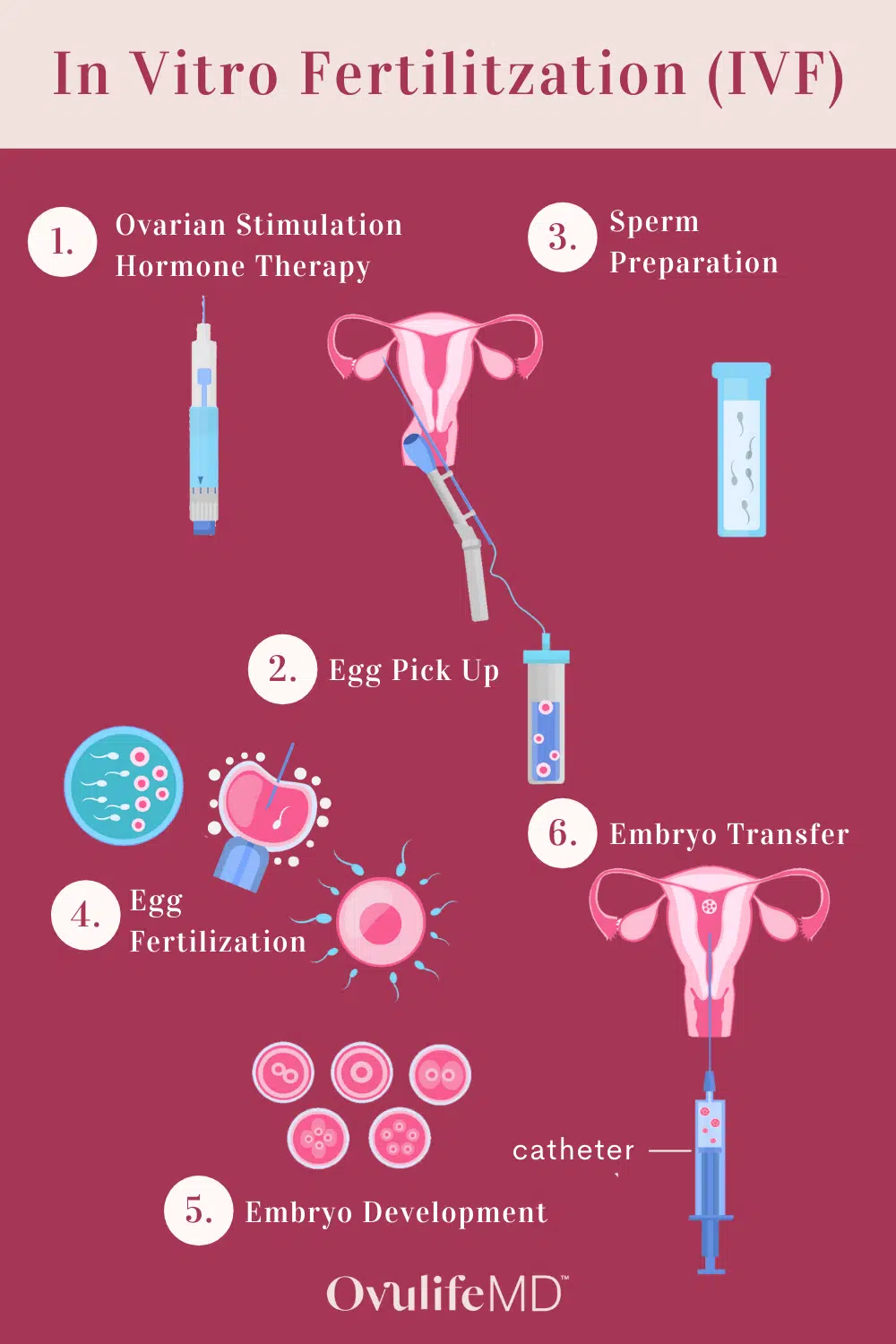
In vitro fertilization or IVF, is a process where eggs are surgically retrieved from the female partner and fertilization takes place outside the body in a dish (in vitro).
In contrast to taking a pill by mouth for 5 days, the process of IVF typically involves injectable medications (gonadotropins) for 9-14 days on average. The response to medications is monitored with a combination of transvaginal ultrasounds and serum estradiol levels. Once the follicles reach a certain size a “trigger shot” is given that triggers final egg maturation. The egg retrieval procedure will be scheduled for ~34 – 36 hours later.
Egg retrieval is considered a minimally invasive procedure that is typically performed transvaginally with need aspiration (no incisions needed). All visible follicles in the ovary are aspirated with the needle under ultrasound guidance. The embryologist then obtains the eggs and inseminates them with the sperm in vitro.
The embryos then develop and are either transferred back into the uterus or frozen for later use. Embryos can be transferred on the 3rd, 5th, or 6th day of growth – some labs will transfer up to day 7 as well. You can ask your fertility clinic what their specific practice is to understand what’s best for you.
If you’re looking for a deeper dive on what to expect with the egg retrieval process (before and after) in general be sure to check out this post on egg freezing for more detail.
Fast Facts for IUI and IVF Treatments
Although it’s difficult to make a direct comparison because of the numerous underlying patient factors that can influence the success of one treatment over another, it’s good to have a general understanding of the difference between IUI and IVF in terms of success rates, costs, side effects, and risks.
Success rates
Success rates for both fertility treatment options depend largely on the age of the woman and underlying infertility diagnosis. In-vitro fertilization boasts a higher live birth rate per cycle and ranges from nearly 50% in women under the age of 35 to 3% in women > 42 years of age according to sart.org. It also typically results in a faster time to pregnancy.
In contrast, intrauterine insemination success rates vary based on age and infertility diagnosis. For younger patient populations with otherwise unexplained infertility, the highest chance of pregnancy is ~15-20%, which is cumulative to a point. Meaning after 3-4 IUI cycles you would have ~45-60% chance of pregnancy. After those 3-4 cycles though, success rates start to decline and aren’t much better than continuing timed intercourse or expectant management.
Depending on what source you look at though, intrauterine insemination success rates have been shown to be anywhere from 5-20% per cycle (1, 2). Ask your fertility clinic what their specific rates are for other patients that are similar to you to get a better idea of your chance per cycle.
Since success rates are cumulative over time with IUI, it may take a little longer to achieve pregnancy. With that said, if a woman is young and has an otherwise good ovarian reserve, it can certainly be a great option to start with. On the other hand, some studies suggest IVF is the fastest way to live birth among older women (1).
Cost comparison
Costs vary regionally and by clinic depending on a number of factors but in general, a single intrauterine insemination cycle can range anywhere from as low as $400 to as high as $4000.
In contrast, in-vitro fertilization, including all the medications and procedures can run anywhere from $18,000-25,000 on average.
Be sure to check with your insurance provider to see what is and is not covered. Some patients’ insurance actually requires a minimum of 3 IUI’s prior to being able to qualify for IVF coverage.
Important Side Effects & Risks
Both fertility treatment options are generally considered low risk and well-tolerated.
Common side effects of medications like clomiphene citrate and letrozole include mood swings, breast tenderness, abdominal bloating, and vaginal discharge. The IUI itself is generally well tolerated with minimal risks.
Although a low-risk process, IVF does have a higher risk of ovarian hyperstimulation syndrome (OHSS) and ovarian torsion comparatively. There are also procedural related risks of the egg retrieval to consider including the risk of sedation and the procedure itself (e.g., bleeding, infection, etc.). But, it’s generally low risk and well-tolerated with mild cramping and abdominal bloating afterward.
Another important consideration is the risk of multiple pregnancies. For medications like clomiphene citrate and letrozole, the twin rate has been noted to be around 5-13% whereas the risk of twins with a single embryo transfer from an IVF cycle is 1% or less (3, 4).
Making the Decision Between IUI and IVF
First and foremost, every individual is unique and you should meet with your Reproductive Endocrinology and Infertility specialist and review your history to determine what treatment is best for you.
In general, IUI tends to be a good first option for couples with ovulatory dysfunction, mild male factor infertility, unexplained infertility, or when using donor sperm. IUI can also be helpful for couples with sexual dysfunction or tough travel schedules (sperm can be frozen in advance for use in case of travel during the fertile window).
Since fertilization is occurring within the body there are a few requirements to be a candidate for IUI including patent (open) fallopian tubes (at least one), having enough sperm (ideally at least 20 million total motile sperm prior to the IUI prep), and working ovaries.
Some couples prefer to start with IUI because it’s less invasive, less expensive, and considered to be a more “natural” way of conception.
However, if patients don’t meet the minimum requirements for IUI to be worthwhile, it may be better to consider IVF from the start.
Common indications for IVF include:
-

Tubal factor (having blocked or nonfunctional fallopian tubes)
-
Severe male factor infertility
-
Concern about passing on certain genetic disorders to offspring
-
Need for donor egg
-
Lack of success with IUI
Of course, things like age, underlying infertility diagnosis, and overall family building goals (how big you want your family to be) are also factors to consider in determining which treatment might be the best place to start for you. For example, if you’re 38 and want 3 children, IVF would offer the best chance of achieving that goal in the future. If you’re 35 and only want one child, IUI could be a great place to start.
When should you move to IVF from IUI?
For most patients, it’s recommended to move forward with IVF after 3-4 cycles of ovulation induction + IUI as success rates start to decline thereafter. There’s no hard and fast rule here though as every patients’ circumstance is different… Maybe you’re using donor sperm or have ovulatory dysfunction or maybe IVF is too pricey and IUI is the primary option… These may be reasons to do a few extra cycles as opposed to halting fertility treatment altogether.
When should you choose IVF instead of IUI?
As noted above, we recommend you discuss your unique circumstances and family-building goals with your reproductive medicine specialist from the start and seek care sooner than later if you’ve been trying to conceive for some time.
With that said, some common reasons to choose IVF instead of IUI include severe male factor, tubal factor, advanced endometriosis, advanced maternal age, decreased ovarian reserve, and desire to avoid passing on certain genetic diseases.
Final Thoughts for Patients Facing Fertility Treatment
If you’ve been trying to conceive for > 12 months and you’re under 35 years of age OR you’re 35 years of age or older and you’ve been trying for 6 months, reach out to a board-certified fertility specialist to have a basic evaluation completed. From there you can discuss potential treatment options including things like IUI or IVF.
It’s important to remember that every individual’s circumstances are unique as is each individual’s fertility journey. Remember to take care of yourself, educate yourself about your options, and be empowered to make informed decisions that are right for YOU.
Resources:
-
Goldman MB, et al. A randomized clinical trial to determine optimal infertility treatment in older couples: the Forty and Over Treatment Trial (FORT-T). Fertil Steril 2014; 101:1574-81.
-
Reindollar RH, et al. A randomized clinical trial to evaluate optimal treatment for unexplained infertility: the fast track and standard treatment (FASTT) trial. Fertil Steril 2010;94:888-99.
-
Diamond MP, et al. Letrozole, gonadotropin, or clomiphene for unexplained infertility. J Engl J Med 2015;373:1230-40.
If you enjoyed this post, get more like it
Always evidence-based. Always actionable.
And just like a good doctor’s visit, your privacy is protected
Don't worry, you can always unsubscribe with just one click.Welcome to the tribe!
You’ve joined the OvulifeMD community. Don’t forget to check your inbox for a special welcome email.
Featured Content




Leave a comment
If you have any questions, we will be happy to answer them.
Thanks for sharing what's on your mind!
Check the thread for more insight and support.