
Genetic testing has become more common as direct-to-consumer tests have become increasingly available. There are more options in the doctor’s office as well, particularly when it comes to fertility treatment and pregnancy care. And while it seems like there is a new test coming out every other week, or some new service being advertised, before you go ordering them all, it’s important to understand what each of them means for your and your baby’s health and when they should be considered. The good news is we’re going to break it all down here!
Here’s a quick overview of what you’ll discover:
What is genetic testing?
Genetic testing is a broad term that can be applied for a variety of different types of genetic tests that fundamentally have one thing in common: examining human DNA to identify changes in genes, chromosomes, or proteins that may help determine a pathologic or disease state.
Although genetic testing can provide critical information for diagnosing and treating certain disorders in both you and your baby, the technology isn’t perfect. Speaking with your physician and genetic counselor about your specific genetic results is critical to have a detailed understanding of what the test results actually mean for your health and the clinical implications before or during pregnancy and for your baby.
One of the most common questions and areas of confusion we’ve noticed with patients is in understanding what exactly each different genetic test is testing, what the results potentially mean especially in the prenatal period, and how they link together if at all.
For the purposes of this blog, we’ll be focusing on common genetic testing scenarios in the fertility world– although the multitude of tests expands far beyond this.
What are the different types of genetic tests and genetic screening?
Genetic Carrier Tests- Expanded Carrier Screening
Carrier screening is a type of genetic test that can tell you if you are a carrier for a certain genetic condition. Carriers for autosomal recessive genetic conditions (what is typically screened for with carrier screening) carry a single copy of the defective gene, therefore they often have no symptoms of the genetic condition or impact on their health because their one normal functioning copy can pick up the slack.
However, if the other biologic parent is also a carrier for the same genetic disorder (cystic fibrosis for example), then their baby would have a 25% chance of inheriting both defective copies of the genes from either parent and thus having the full mutation and expression of the genetic disease state.
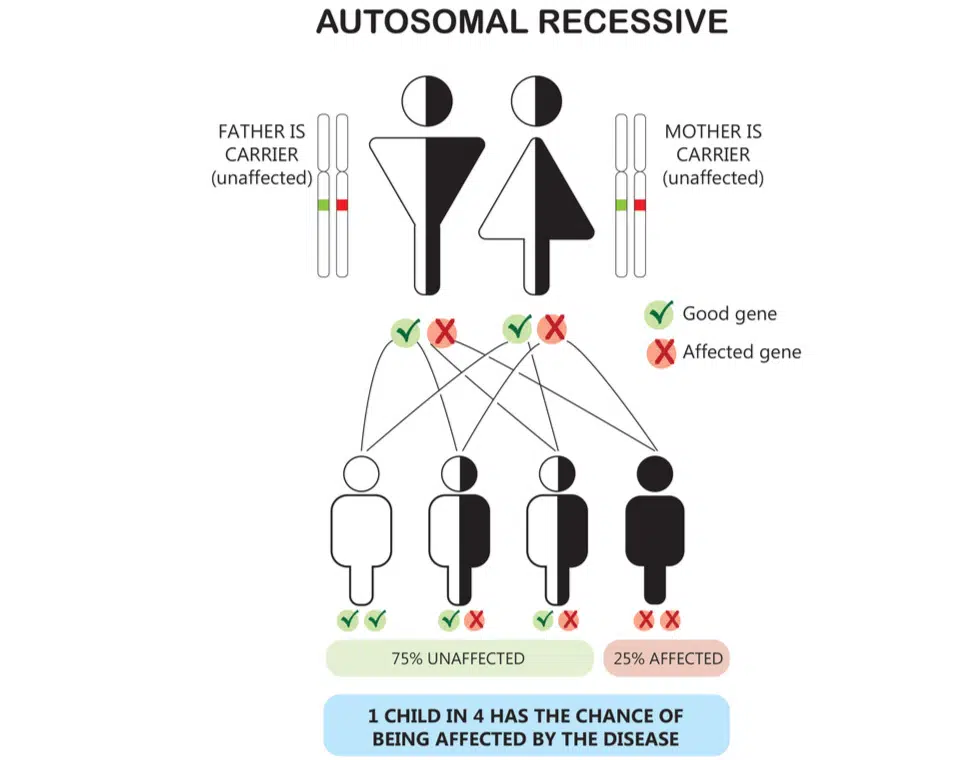
So to recap, for autosomal recessive conditions it takes two genes, one inherited from each biological parent, to have a recessive genetic disorder. Since carriers often have no symptoms or health-related effects a genetic carrier test is recommended prior to pregnancy so couples can better understand their reproductive risk and options for their future baby (1). Typically screening starts with the biological mother. If the biological mother is found to be a carrier for a certain genetic disorder then testing of the biological father is recommended to assess for the same genetic disorder.
If both partners are found to be carriers of the same disorder, genetic counseling should be recommended as there are different reproductive options to consider including things like preimplantation genetic testing for monogenetic defect (PGT-M) versus diagnostic testing in pregnancy like amniocentesis.
Understandably, in a recently updated article, the American College of Obstetricians and Gynecologists advise that: “information about genetic carrier screening should be provided to every pregnant woman…” and “…ideally before pregnancy” so couples understand their baseline risk and options prior to conception or delivery (1).
Of note, there are different types of carrier screening panels available ranging from testing for a single autosomal recessive condition to a limited carrier panel including just the most common autosomal recessive conditions (like cystic fibrosis, spinal muscular atrophy, etc), up to nearly 300 conditions (expanded carrier screening). Often, the cost is the same no matter how many genetic conditions are being assessed so ask about that before choosing which panel you want.
Be sure to understand which genetic test you are getting and what all is being screened for to be able to make the most informed decision and ask your physician about preconception carrier screening even if you’re already pregnant.
What are some of the most common genetic diseases?
As mentioned above, there are both limited and expanded carrier panels. Limited panels typically include autosomal recessive disorders that are more common in the general population. Carrier frequencies typically vary by race and ethnicity as well and that’s important to note to understand the potential health risk to your future baby.
Cystic Fibrosis
Classic cystic fibrosis (CF) is an inherited disorder that causes significant damage to the lungs and digestive system. It is the most common life-threatening autosomal recessive condition amongst non-Hispanic white individuals (carrier frequency of 1 in 25 individuals) that can result in debilitating respiratory symptoms, which is the most common cause of death. ACOG recommends screening for cystic fibrosis should be offered to all women who are considering pregnancy or are currently pregnant regardless of family history (1).
Spinal Muscular Atrophy
Spinal muscular atrophy (SMA) is a neuromuscular disorder that causes muscles to become weak and atrophy (waste away). There is wide variability in symptom severity of this disease ranging from the weakness of voluntary muscles (for arm and leg functioning) to the muscles used to breathe and swallow which can have devastating consequences. This occurs in approximately 1/6000–10,000 live births and is the greatest genetic cause of infant death. Carrier frequencies vary from 1 in 35 in caucasian individuals to 1 in 117 in Hispanic individuals. ACOG recommends screening for spinal muscular atrophy should be offered to all women who are considering pregnancy or are currently pregnant (1).
Sickle Cell Disease
Sickle cell disease belongs to a group of autosomal recessive conditions that have an abnormal hemoglobin structure (hemoglobinopathies). Sickle cell has altered hemoglobin S which causes the blood to “sickle” (hence the name) resulting in a variety of symptoms related to the constriction of blood vessels which are often extremely painful, known as sickle cell disease. Sickle cell is the most common in individuals of African origin with approximately 1 in 10 having sickle cell trait, and 1/300-500 having some form of sickle cell disease.
Thalassemia
The thalassemias are another form of hemoglobinopathy whose pathology is characterized by abnormal production of hemoglobin with varying health symptomatology and presentation depending on which globin chain is involved. Alpha and beta thalassemias are the most common. Accurate detection and characterization of hemoglobinopathies often involve additional blood tests including a complete blood count (CBC) and hemoglobin electrophoresis. These are more common in individuals of African, Mediterranean, Southeast Asian, West Indian, and Middle Eastern descent.
Carrier Screening Summary
In summary, carrier screening should be offered to all couples contemplating pregnancy and to women who are pregnant if it wasn’t completed prior to pregnancy. If carrier screening is completed prior to pregnancy and a couple is found to be carriers of the same condition, that affords the opportunity to consider all of their options, prior to being faced with having to make critical decisions during pregnancy if both genes are inherited by their baby. One of the options would include undergoing in vitro fertilization and screening embryos for the same condition via preimplantation genetic testing (PGT) prior to embryo transfer. More on that below…
Preimplatation genetic testing (PGT)
PGT is a type of genetic screening that can be performed on embryos in individuals who have undergone in vitro fertilization (IVF) prior to embryo transfer and pregnancy. Once the embryo grows to the blastocyst stage (a day 5 or 6 embryo), approximately 5-10 cells can be biopsied off the trophectoderm (what will eventually become the placenta) and sent for genetic testing.
There are a variety of technologies available for PGT, which continue to rapidly evolve but three types of PGT testing are currently used:
-

PGT-A (aneuploidy)
-
PGT-M (monogenetic defects)
-
PGT-SR (structural rearrangement)
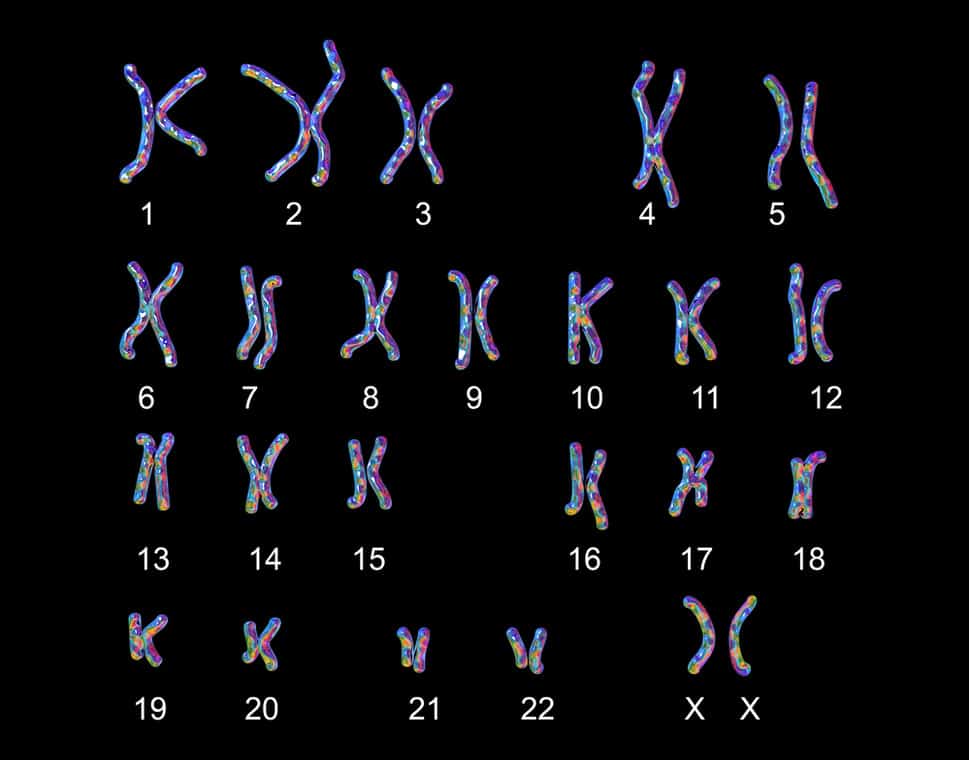
PGT-A (formerly known as preimplantation genetic screening or PGS) is the most common form of PGT and is used to assess the chromosome copy number of the embryo prior to an embryo transfer. A “euploid” embryo is one that contains 2 copies of each chromosome (one inherited from each parent) resulting in 46,XX or 46,XY karyotype.
Aneuploid embryos or ones that are missing certain chromosomes or have an extra chromosome are “imbalanced” and often won’t result in pregnancy or a healthy baby, and will result in a negative pregnancy test or an early miscarriage. The likelihood of having an aneuploid or chromosomally imbalanced embryo increases with advancing maternal age.
PGT-M can be used alone or in combination with PGT-A to assess if an embryo is affected by a certain genetic disorder prior to pregnancy. Going back to some of the examples we discussed earlier with carrier screening, if two parents were both found to be carriers of cystic fibrosis (CF), PGT-M would be an option if they wanted to screen the embryo for cystic fibrosis genes before embryo transfer and pregnancy. If they were both carriers and underwent IVF and had four embryos available for embryo transfer, one out of the four tested would be affected by CF. Therefore, PGT-M could be utilized to ensure the transfer of an unaffected embryo.
PGT-SR is utilized for embryos with known parental balanced chromosomal translocations or inversions that have resulted in repetitive miscarriages or recurrent pregnancy loss. Parental karyotype analysis is part of the recommended workup for recurrent pregnancy loss (more on that below). If a parent is found to have a balanced translocation or inversion, PGT-SR may be utilized to reduce the risk of repeat miscarriage due to chromosomal abnormalities.
Now it’s important to note here that all PGT tests are considered screening tests, not diagnostic. And nothing guarantees the delivery of a healthy baby. In other words, they can detect chromosomal copy numbers with a high level of accuracy but false positive and false negative tests can occur. Additional diagnostic testing during pregnancy (via amniocentesis, or sampling some of the amniotic fluid) may be indicated depending on the scenario.
Parental Karyotype
As noted above, obtaining a karyotype on the biological parent is part of the recommended evaluation for recurrent pregnancy loss. Karyotype analysis is typically performed by a blood sample and assesses both chromosome copy number and structure. Some individuals may have balanced translocations or inversions of genetic material resulting in no obvious symptoms for them, but when their genetic material goes to recombine with their partners, it does so unevenly and can lead to an increased risk of miscarriage… which is where PGT-SR may be helpful. This test may also be indicated if someone in your family has had a karyotype consistent with a tranlocation or inversion of genetic material.
When should I consider genetic testing- before or after I’m pregnant?
This is a great question, and as you can tell from the sections above, it all depends on where you are in your journey.
-
For carrier screening, it is recommended to consider screening prior to or during pregnancy… so if you’re even contemplating getting pregnant, there’s no better time than the present. Or maybe you recently conceived– great! Speak with your doctor about your options to optimize long-term health outcomes.
-
If you and your partner are both carriers for the same autosomal recessive condition or if you have another hereditary disorder or disease in your family, PGT-M may be considered prior to pregnancy. If you choose not to go the route of IVF or that isn’t an option, other prenatal genetic testing is also available to assess the genetic or disease carrier status of the pregnancy once you are already pregnant.
-
If you’re already undergoing IVF for other reasons, PGT-A may be recommended to reduce the risk of miscarriage due to aneuploidy.
-
If you’ve been diagnosed with recurrent pregnancy loss a karyotype should be considered and depending on the results, PGT-SR may be recommended as well.
-
If you are already pregnant, there are two main types of prenatal genetic testing available: 1) screening tests (noninvasive- with a maternal blood sample and ultrasound) versus 2) diagnostic tests (where cells are obtained directly from the placenta or fetus through chorionic villus sampling (CVS) or amniocentesis). The trimester prenatal testing or prenatal screening is completed in depends on the test being performed.
When does my family health history matter for genetic screening with pregnancy?
It’s also important to take your family health history into account when considering preconception genetic testing. We already discussed autosomal recessive diseases (meaning you have to inherit two copies of the defective gene to be affected). Screening you and/or your partner is also important if someone in your family or their baby is affected by certain genetic disorders or they’ve had a genetic carrier status screening in the past and know they’re positive. Having a sibling, cousin or other family members (even if a distant relative) that has an affected child would be another indication to screen you for the same condition or disease.
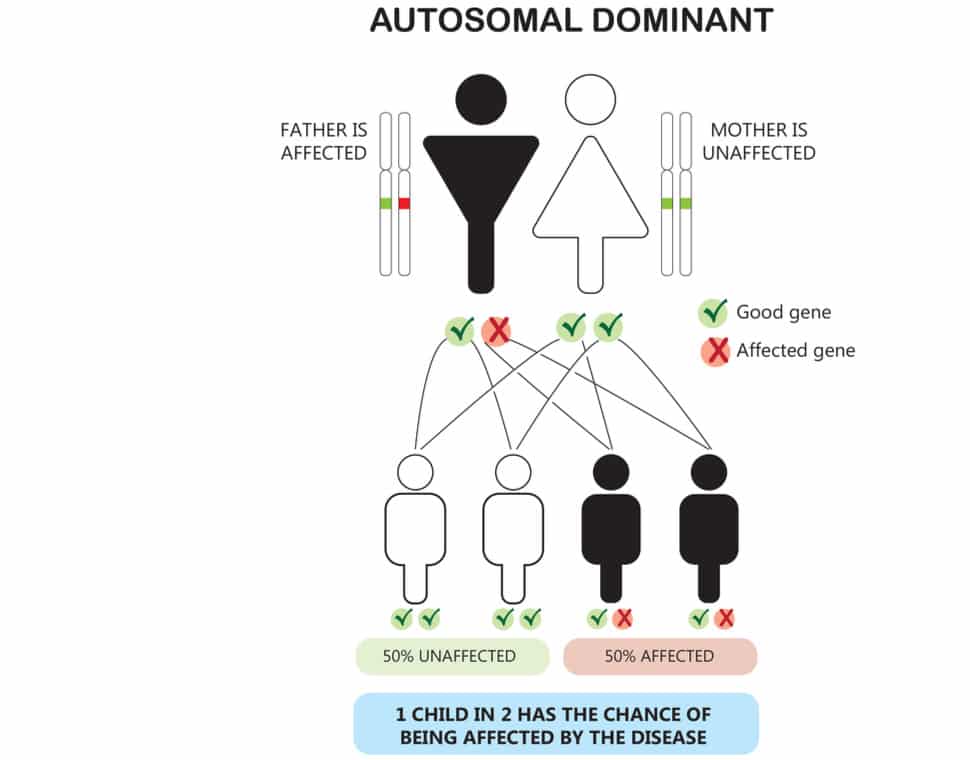
It’s also important to know if an autosomal dominant condition or disease exists in your family. In contrast to autosomal recessive conditions, autosomal dominant conditions just require one copy of the gene to be inherited to potentially be affected. Examples of autosomal dominant conditions include things like neurofibromatosis (NF), Huntington’s disease, Marfan’s, and BRCA (the breast cancer gene) among others which can have significant health implications. If anyone in your family has one of these conditions, speak with your doctor about it.
Final Thoughts
As you can see, “genetic testing” is a bit of a catch-all term that can get a little confusing and can go by many different names. We hope the information provided here at least sheds a little more light on what “genetic testing” we’re commonly referring to in the fertility world and what you should consider getting tested for.
Carrier screening, preimplantation genetic testing, and karyotype analysis are all distinctly different tests available with different indications. And while none are necessarily required, or guarantee the health of your baby, this area of medicine continues to rapidly evolve, with new tests becoming available all the time. Be sure to speak with your OB GYN about you and your family history before you pay for an external, direct-to-consumer test to discuss which ones are right for you and worth your money.
P.S. Be sure to check out one of our prior blog topics if you want a deeper dive into other infertility facts and statistics
References:
-
The American College of Obstetricians and Gynecologists. Committee Opinion Number 691. Carrier Screening for Genetic Conditions. March 2017.
If you enjoyed this post, get more like it
Always evidence-based. Always actionable.
And just like a good doctor’s visit, your privacy is protected
Don't worry, you can always unsubscribe with just one click.Welcome to the tribe!
You’ve joined the OvulifeMD community. Don’t forget to check your inbox for a special welcome email.
Featured Content




Leave a comment
If you have any questions, we will be happy to answer them.
Thanks for sharing what's on your mind!
Check the thread for more insight and support.