
Infertility is a tough journey to navigate
(Understatement implied).
So many questions…
So much time spent waiting…
So much time is spent wondering…
“What is actually working?”
“How can I make it better?”
And Dr. Google is abundant with information and advice that often directly conflicts with what your doctor says… meaning it’s hard to know fact from fiction, making everything that much more frustrating on your journey.
Instead of getting frustrated and overwhelmed, we wanted to cover some of the most frequently asked questions about causes of infertility in females and what you CAN be doing to help optimize your health and fertility – no matter where you are in your journey 🙂
We’ll also touch on how to find a qualified health care provider in your area if you’re struggling with where to start. And even if your fertility journey hasn’t begun yet, we hope that the information covered here is informative and empowering for you or someone you know.
Here’s a quick overview of what you’ll discover:
Important Facts to Understand About Infertility for Women
Infertility is generally defined as the inability to conceive after one year of having regular, unprotected sex if the female partner is < 35 years of age, or after 6 months if ≥ 35 years of age.
And even though approximately 1 in 8 couples will be diagnosed with infertility, roughly 85% of couples will get pregnant within 1 year of trying (1).
That means the probability of getting pregnant in a single menstrual cycle (i.e., fecundability) is 20-25% at best… which, unfortunately, is lower than most people think.
Then you have to take into account the baseline risk of miscarriage, which can range from 10-15% risk for a woman in her 20s to >50% chance for a woman in her mid-40s. Hence, why maternal age is such an important factor.
Despite being a complete annoyance, it’s essential to understand how age relates to fertility as this can better guide you on when it’s time to seek care from a fertility specialist. With that said, there are special circumstances where it might be better to seek care sooner rather than later, even if you haven’t been trying to conceive for six months to a year.
More on that below…
What Causes Female Infertility?
The causes of female infertility are varied.
Sometimes it can be a single factor that can be easily treated, while other times it might be caused by a combination of multiple factors.
Some of the most common causes of female factor infertility include ovulatory dysfunction, tubal factor, and unexplained infertility.
You’ll notice the discussion of male factor is outside of the scope of this blog… but don’t forget that decreased sperm counts account for nearly ⅓ of cases of infertility. So, if you’re getting checked out… make sure your man gets a sperm count too!
While this list isn’t all-encompassing, we’ll dive a little deeper into each of these more common fertility problems. Remember, taking into account a woman’s specific health history is the most important part of starting the evaluation and making an accurate diagnosis… because we’re all different after all!
Ovulatory dysfunction
Ovulatory dysfunction, or not releasing an egg in a patterned timely fashion each month (ovulation), causes infertility 20-40% of the time for females. (1)
Normal menstrual cycle length (the time from cycle day 1 of menses to your next cycle day 1 of menses) is 21 – 35 days lasting on average for 5 days (2).
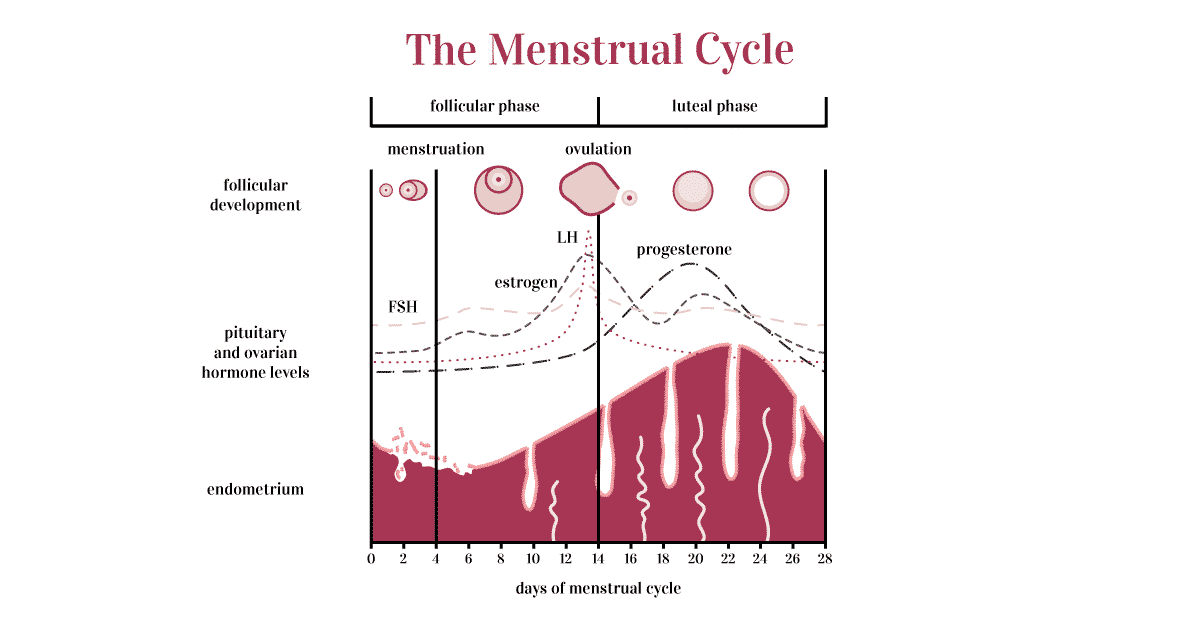
Only 20% of women actually have a 28-day cycle which is what is traditionally considered ‘normal.’ And even though 21 – 35 days may seem like a wide range, what’s most important is actually the regularity from one cycle to another.
That means if you have 22-day cycles – which may seem on the shorter side of normal – AND they consistently occur every 22 days (± 1 day), then your cycles should not cause problems and they denote regular ovulation.
On the other hand, if your cycles are < 21 days, > 35 days apart or irregular (varying by more than 4-5 days from one cycle to another), or if they are overall unpredictable or infrequent, you likely have ovulatory dysfunction (i.e., lack of timely ovulation each month).
Reviewing a woman’s menstrual history alone is typically adequate to accurately diagnose ovulatory dysfunction.
Treatment certainly depends on the cause but it’s important to start with any underlying causes that are easily correctable.
Common endocrine disorders such as thyroid issues (hypothyroidism or hyperthyroidism) can cause dysregulation in the signaling from the brain to the ovary and lead to ovulation problems. Elevation of a hormone called prolactin can cause the same. Often times once treated, that will be sufficient to achieve regular ovulation and pregnancy.
Polycystic ovary syndrome (PCOS) is a common condition that affects 1 in 10 reproductive-age women and can result in a complete lack of ovulation or vastly erratic menses. Menstrual cycle variability is just one part of the diagnostic criteria for PCOS, so it’s important to speak with your healthcare provider if you are experiencing other symptoms that make you concerned about PCOS.
There are different ways to try and track ovulation such as basal body temperature, cervical mucus testing, and ovulation predictor kits (LH kits), but a serum progesterone level one week after ovulation is confirmatory – a level > 3 ng/mL is consistent with ovulation.
If ovulatory dysfunction is otherwise unexplained often, inducing ovulation with a medication like clomiphene citrate (Clomid) or letrozole (Femara) will be minimally invasive and highly effective at achieving pregnancy.
Tubal factor
Tubal factor is one of the most common causes of female infertility and impacts approximately 30-40% of women (1). Tubal factor female infertility is caused when the fallopian tubes are blocked which prevents the sperm from meeting the egg… thus the egg can’t be fertilized by sperm.
Risk factors for tubal factor infertility include a history of sexually transmitted infection (e.g., chlamydia and/or gonorrhea) or pelvic inflammatory disease, history of a ruptured appendix, or other major abdominal or tubal surgery that resulted in surgical trauma. Endometriosis may also impact tubal function (more on that below).
Hysterosalpingogram (HSG) or saline infusion sonogram (SIS) are common methods to screen for fallopian tube causes of infertility but laparoscopy (abdominal surgery) with direct visualization of the tubes being filled with dye is diagnostic.
The type of blockage is also important to consider.
Is the tube simply blocked? Or is it swollen, dilated, and filled with inflammatory fluid (i.e., a hydrosalpinx)? Are one or both tubes blocked? Are you at an increased risk of ectopic pregnancy (i.e., getting pregnant but having it implant in the fallopian tube)?
If just one tube is blocked and the other appears normal, then more conservative treatment may still be an option. And depending on the area and type of blockage (if the blockage is closer to the uterus) cannulation to open up the blocked area might be considered.
Historically surgery to evaluate for and remove any pelvic adhesive disease (i.e., scar tissue) around the tube was routinely recommended. However, due to the increasing success rates of other advanced reproductive treatments, this is generally recommended less frequently.
If both tubes appear to be blocked or have severe adhesive disease, then in vitro fertilization (IVF) a form of assisted reproductive technology (ART) is an extremely effective treatment option that bypasses the fallopian tubes entirely. This is also often recommended if there is a significant decrease in sperm counts that would prevent an egg from being fertilized conventionally.
Understanding specifically the type and location of the tubal blockage in the context of a woman’s specific health history is integral in helping you have the best grasp of what the treatment options are and what is likely to be most effective.
Unexplained Infertility
After a standard infertility workup, approximately ⅓ of couples will be diagnosed with unexplained infertility. This diagnosis typically includes a normal semen analysis for the male partner, at least one patent (open) fallopian tube, and documentation of normal ovulation for the female partner.
This can be one of the most frustrating diagnoses because…
If everything is “normal”, then what isn’t working?
Or what caused this to happen?
The reality is that so much has yet to be discovered in the field of reproductive medicine.
However, the good news is that treatment options for unexplained infertility have been well studied and are fairly effective. They include ovarian stimulation (to boost the number of eggs released each month) with intrauterine insemination (IUI) or advanced reproductive treatments such as IVF. Moreover, a large percentage of couples with unexplained infertility will eventually conceive on their own relative to other infertility diagnoses.
Which treatment to pursue with unexplained should take into account:
-

The age of the female partner
-
Desired family size.
Data has shown that ovarian stimulation with intrauterine insemination for 3-4 cycles will optimize the chances of pregnancy depending on a woman’s age. It’s also important to note that IUI alone or ovarian stimulation with oral medication (or less frequently injectable gonadotropins) alone is less effective than the combination of the 2 treatments concurrently and is no more effective than expectant management (unexplained infertility ASRM reference 3-5).
So let’s review that again…
Ovarian stimulation with oral medications + IUI is more effective than ovarian stimulation or IUI alone… both of which in isolation aren’t any more effective than trying on your own with unexplained infertility.
For women > 37 years of age, data has also shown that IVF is likely the fastest way to live birth with a lower cost per pregnancy compared to starting with ovarian stimulation and IUI which can in part be attributed to the decrease in egg quality as we age (6). However, due to added cost and invasiveness, IVF may not always be a realistic treatment option for all women. In which case, ovarian stimulation with IUI is a great place to start and can still significantly help increase your chances of getting pregnant.
Endometriosis
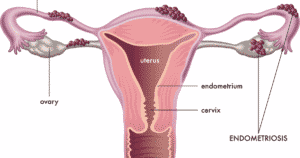
Endometriosis is the implantation of endometrial tissue outside of the endometrial cavity. Endometriosis is a common cause of chronic pelvic pain in women but may also be asymptomatic.
It has been suggested that anywhere from 25-50% of women with infertility have endometriosis and that 30-50% of women with endometriosis have infertility (7). The incidence is as high as 80% in women with chronic pelvic pain (1).
So what’s the connection?
Although the true impact is still debated amongst specialists, there are a variety of ways endometriosis may contribute to infertility.
More severe cases of endometriosis can cause significant anatomic distortion of critical pelvic organs as well as tubal scarring and swelling of the fallopian tubes which could result in tubal factor infertility from pelvic adhesive disease as noted above.
Other mechanisms that have been proposed include a negative impact on egg and embryo quality, inflammation, abnormal tubal transport (even if the tubes are open), endocrine abnormalities, and impaired implantation. Each of these potential mechanisms is well summarized in ASRM’s Committee Opinion on Endometriosis and Infertility. (8)
But if there are so many potential mechanisms by which endometriosis can negatively affect fertility and such a high prevalence of it in a reproductive age population of women… why does it take on average 7 years to diagnose? (9)
Well, for one, endometriosis requires surgery to diagnose with confirmation of the pathology of a biopsy or specimen removed during surgery. So given that surgery is invasive and can be expensive, it’s not always the first line especially if symptoms are mild.
Treatment options include medications for pain management or hormonal suppression or surgery to remove the endometriosis. When it comes to fertility treatment options, generally the options are similar for unexplained infertility if tubal patency is confirmed, but some studies have suggested IVF is the most effective treatment option to achieve pregnancy in this patient population. Whether or not surgery is indicated or will help prior to treatment is widely debated.
The reality is, is that many factors play into what might be the best treatment option with endometriosis… female age, presence or absence of pelvic pain, how severe the pain is, duration of infertility, and how severe the endometriosis appears to be.
If you have a long-standing history of chronic pelvic pain that worsened after coming off birth control, pain that increases prior to menses, pain with bowel movement or with intercourse, it’s important to know these symptoms are NOT normal and they are something you should speak with your OB/GYN or infertility doctor about it.
If you don’t feel like you’re being heard, be empowered to get a second or a third opinion from another doctor.
Thankfully, endometriosis and related pain is generally suppressed during pregnancy… so getting pregnant can help!
Other causes of female infertility to consider
Beyond ovulatory dysfunction, tubal factor, unexplained infertility, and endometriosis there are certainly other causes of female infertility to consider.
Uterine fibroids are a common cause of heavy menses in women and depending on the side and locations of the fibroids could certainly impact fertility (uterine factor). A simple pelvic ultrasound is an easy way to assess for fibroids or for other uterine causes.
Other anatomic abnormalities along the endometrium should be considered such as endometrial polyps which can typically be diagnosed on the imaging obtained to evaluate the fallopian tubes we discussed above (HSG or SIS).
Advanced maternal age may also be a contributing cause with the likelihood of spontaneous pregnancy above the age of 45 approaching 0% due to a decrease in egg quality over time (the genetic content of eggs).
And of course, there is male infertility. Reduced sperm counts or male factor contributes to infertility nearly half of the time and is the sole factor nearly ⅓ of the time… so getting a semen analysis as a baseline part of the workup is often ignored but is essential!
Female Infertility Treated… What Are Your Options?
Treatment certainly depends on the underlying cause.
If it’s isolated ovulatory dysfunction an oral medication to induce ovulation may be all that is needed.
If caused by a mild male factor or unexplained infertility, the addition of IUI may be recommended.
If severe tubal factor is noted, then IVF may be the primary option or recommendation.
If fibroids or other uterine factors are diagnosed, surgery may be recommended.
If it’s strictly age-related, and treatment with a woman’s own eggs isn’t an option perhaps donor egg, donor embryo, or adoption should be considered.
As ART has improved immensely over the past decades, IVF has become the most effective treatment option for nearly all causes of infertility (including severely decreased sperm counts), but unfortunately is more invasive and costly.
There are so many beautiful ways to build a family and there is no single right way to go about it. Ultimately you should be fully informed about your unique scenario and understand the treatment options available and their success rates so you can make the most informed decision for yourself.
We hope this blog gives you a little insight into the different causes, the workup, and treatment options available for the different types of female infertility.
How To Optimize Your Overall Health to Boost Fertility and Improve Infertility Treatment Outcomes
Depending on your insurance coverage, infertility treatment is costly, no matter which route you take. That means it’s important to do everything we can to optimize our overall health and increase our chances of success before or even during infertility treatment.
Luckily, there are many lifestyle factors that have been scientifically proven to have a significant impact on your reproductive health… (for both eggs and sperm!) And when working with our patients we always focus on three key areas:
Overriding fertility threats.
Vitalizing and nourishing the body.
Uniting the mind-body connection.
The OvuMethod is actually our integrative approach to naturally optimizing fertility and women’s health overall. It’s a complete system. We’ll quickly summarize each of these steps so you can start taking action today to optimize your fertility and overall health today.
Overriding fertility threats is all about removing the toxins that are harming our bodies. Whether that be the food we eat or chemicals in our environments, it’s critical to minimize exposure to these toxins when possible.
Vitalizing and nourishing the body is focused on fueling our bodies with pro-fertility foods and moving our bodies. There are many unique aspects of a true fertility diet that goes beyond “just eat healthy” that should be considered.
Uniting the mind-body connection is one of the most important steps on any woman’s fertility journey. Your mental health is every bit as important as your physical health. Practicing mindfulness, tuning into your body’s and mind’s needs, and finding peace amongst the periods of waiting and unknown is vitally important to your wellbeing.
When addressing each of these three pillars, not only are you optimizing your overall health and wellbeing, but also the health of your egg, sperm, and future pregnancy.
If any aspect of this approach resonates with you, we invite you to check out our program Nourish Your Fertility, to help put some of these impactful changes into action.
Final Thoughts on Infertility in Women
Infertility in women is far more common than people think and there are some common causes that are important to consider based on your unique health history. We hope this helped provide an overview of common causes and treatments to consider as a woman struggling with infertility.
Don’t forget though… over half of the time male factor infertility due to decreased sperm counts can also play a role and should definitely be evaluated! We promise to dedicate another blog post soon to all things sperm and male factor.
Information is power.
If you are unsure of where to start and you’re looking for a fertility doctor check out the Society for Assisted Reproductive Technology (SART) to find a clinic in your area. See what services they offer and what their lab success rates are. You can also identify physicians that are double boarded (credentialled) specifically infertility and reproductive medicine (which is so important)
And remember, no matter where you are on your journey to focus on what you can control, such as optimizing nutrition and your overall health, minimizing toxin exposure, and finding peace within the chaos.
P.S. Be sure to check out our reference list which can help you find a study that takes a deeper dive into many of the topics we discussed above!
References:
-
Fritz, M. A., & Speroff, L. (2011). Clinical gynecologic endocrinology and infertility (8th ed.). Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins.
-
ACOG Practice Bulletin. Diagnosis of abnormal uterine bleeding in reproductive-aged women. Number 128. July 2012.
-
Guzick DS, Carson SA, Coutifaris C, Overstreet JW, Factor-Litvak P, Steinkampf MP, Hill JA, Mastroianni L, Buster JE, Nakajima ST, Vogel DL, Canfield RE. Efficacy of superovulation and intrauterine insemination in the treatment of infertility. National Cooperative Reproductive Medicine Network. NEJM 1999;340:177–83.
-
Chaffkin LM, Nulsen JC, Luciano AA, Metzger DA. A comparative analysis of the cycle fecundity rates associated with combined human menopausal gonadotropin (hMG) and intrauterine insemination (IUI) vs. either hMG or IUI alone. Fertil Steril 1991;55:252–7.
-
Serhal PF, Katz M, Little V, Woronowski H. Unexplained infertility–the value of Pergonal superovulation combined with intrauterine insemination. Fertil Steril 1988;49:602–6.
-
Reindollar RH, Regan MM, Neumann PJ, Levine BS, Thornton KL, Alper MM, et al. A randomized clinical trial to evaluate optimal treatment for unexplained infertility: the fast track and standard treatment (FASTT) trial. Fertil Steril 2010;94:888–99.
-
Missmer SA, Hankinson SE, Spiegelman D, Barbieri RL, Marshall LM, Hunter DJ. Incidence of laparoscopically confirmed endometriosis by demographic, anthropometric, and lifestyle factors. Am J Epidemiol 2004;160: 784–96.
-
Endometriosis and infertility: a committee opinion. The Practice Committee of the American Society for Reproductive Medicine. Fertil Steril. 2012;98:591-8.
-
Arruda MS, Petta CA, Abrao MS, Benetti-Pinto CL. Time elapsed from onset of symptoms to diagnosis of endometriosis in a cohort study of Brazilian women. Hum Reprod. 2003;18(4)756-759.
If you enjoyed this post, get more like it
Always evidence-based. Always actionable.
And just like a good doctor’s visit, your privacy is protected
Don't worry, you can always unsubscribe with just one click.Welcome to the tribe!
You’ve joined the OvulifeMD community. Don’t forget to check your inbox for a special welcome email.
Featured Content




Leave a comment
If you have any questions, we will be happy to answer them.
Thanks for sharing what's on your mind!
Check the thread for more insight and support.